The officers, Lawrence Manzi and Emmanuel Rusingizandekwe, graduated with the rank of Assistant Inspector of Police (AIP).
The graduation ceremony was held on Friday in Singapore.
The event was attended by the High Commissioner of Rwanda to Singapore, Innocent B. Muhizi, Rwandan diplomats in Singapore, and ACP Augustin Ntaganira, Deputy Commandant and Chief Instructor at the National Police College in Musanze.
The training forms part of ongoing institutional cooperation between the two police forces aimed at strengthening professional development and capacity building for officers.
Rwanda–Singapore cooperation
Rwanda and Singapore maintain strong bilateral relations rooted in cooperation in governance, innovation, and institutional development.
The current security partnership was formalised in August 2022 and includes training and capacity building, exchange of expertise, information sharing, and coordination in addressing transnational crimes such as cybercrime and money laundering.
Beyond security cooperation, the two countries collaborate in ICT, innovation, education, and public sector transformation. Rwanda has also drawn inspiration from Singapore’s development model, particularly in economic transformation, digital governance, and efficient public service delivery.
Singapore has supported Rwanda’s efforts to develop its digital economy, including initiatives in financial technology (Fintech) and innovation-led growth.
The officers, Lawrence Manzi and Emmanuel Rusingizandekwe, graduated with the rank of Assistant Inspector of Police (AIP).The event was attended by the High Commissioner of Rwanda to Singapore, Innocent B. Muhizi, Rwandan diplomats in Singapore, and ACP Augustin Ntaganira, Deputy Commandant and Chief Instructor at the National Police College in Musanze.The training forms part of ongoing institutional cooperation between the two police forces aimed at strengthening professional development and capacity building for officers.
The meeting took place at Urugwiro Village and brought together Daniel Libeskind, Founder and Principal Architect of Studio Libeskind; Nina Libeskind, Co-founder of Studio Libeskind; Stefan Blach, Partner at Studio Libeskind; and Holm Keller, Chairman of the kENUP Foundation.
The planned monument is expected to transform the Kigali Genocide Memorial in Gisozi, where more than 250,000 victims of the 1994 Genocide against the Tutsi are laid to rest, into a powerful space for remembrance, education, and reflection through cutting-edge technology and a deeply immersive, personal visitor experience.
Daniel Libeskind was born in 1946 in Poland to Jewish parents who survived the Holocaust, the Nazi murder of six million Jewish people during World War II. That history is inseparable from his work. Rather than designing buildings that simply house exhibitions, Libeskind engineers the architecture itself into the emotional experience: walls lean, floors tilt, spaces are left deliberately empty. The building becomes the story.
This is the philosophy coming to Gisozi. Here are 10 projects that show what that means in practice:
1. Jewish Museum Berlin (Germany)
This is the project that founded Studio Libeskind and established its global reputation. The titanium-zinc-clad building zigzags across its site, its surface cut by narrow, irregular windows that slash the facade like wounds.
Inside, a series of “Voids”, tall, unheated concrete chambers, cut through the building from basement to roof. Visitors can peer into them from bridges overhead but cannot enter. They represent the absence left by the six million people killed in the Holocaust: the conversations, children, and contributions that no longer exist. The emptiness is the exhibit.
Completed: 2001
Construction cost:$87 million (approx. €60 million)
2. World Trade Center Master Plan (New York City, USA)
On 11 September 2001, nearly 3,000 people were killed when terrorist attacks brought down New York’s Twin Towers. The 16-acre site became the most scrutinised piece of land on earth. After an intense international competition, Libeskind’s “Memory Foundations” plan was selected to guide the rebuilding.
Where others proposed filling the ground with new towers immediately, Libeskind kept the towers’ footprints permanently open, the space that became today’s memorial pools. He also fought successfully to preserve a stretch of original underground slurry wall that had survived the collapse, framing it as a symbol of resilience. It remains visible to visitors at the 9/11 Memorial Museum today.
Completed: 2003 (master plan selected); site construction 2006–2016
Construction cost: Total site redevelopment cost over $20 billion. One World Trade Center alone cost $3.9 billion, making it the most expensive skyscraper ever built in the United States at the time.
3. Imperial War Museum North (Greater Manchester, UK)
During World War II, the Trafford Park area of Greater Manchester, home to factories producing Lancaster bombers and Rolls-Royce aircraft engines, was targeted in the Manchester Blitz. Over two nights in December 1940, 684 people were killed. The Imperial War Museum’s northern branch was built on that same bombed waterfront.
The building is composed of three interlocking aluminium-clad shards representing war on earth, in the air, and on water, fragments of a globe shattered by conflict. Inside, floors curve subtly underfoot and walls lean at unsettling angles. There are no comfortable right angles. The disorientation is deliberate: Libeskind wanted the building itself to produce the instability of wartime before a single exhibit is read.
Completed: 2002
Construction cost: £28.5 million (approx. $40 million). Originally budgeted at £40 million, the project was completed under budget after funding shortfalls led to design economies including substituting metal for concrete in the shards.
4. Military History Museum of the Bundeswehr (Dresden, Germany)
In February 1945, British and American bombers conducted devastating raids over Dresden, creating a firestorm that killed tens of thousands of civilians. Decades later, Libeskind was asked to transform the city’s neoclassical military arsenal, originally completed in 1876, from a glorification of military power into an honest reckoning with war’s costs.
His response was to drive a massive five-storey steel-and-glass wedge straight through the centre of the old building. The contrast between nineteenth-century stone and sharp modern glass is deliberately violent: authoritarian order cracked open. The tip of the wedge points in the direction from which Allied bombers approached on those February nights, a permanent, silent gesture anchoring the building to the city’s defining wound.
Completed: 2011
Construction cost: €48 million (approx. $65 million), funded entirely by the German federal government.
5. National Holocaust Monument (Ottawa, Canada)
Canada’s national Holocaust memorial features six raw concrete volumes that, viewed from above, form a fractured Star of David, the ancient symbol of Jewish identity, broken apart. Visitors move through narrow, oppressive concrete corridors that gradually open upward to the sky: confinement giving way to hope.
The interior walls carry large monochromatic photographs by artist Edward Burtynsky, laser-etched directly into the concrete, haunting wide-angle images of European death camp landscapes. History is not displayed on a panel to be walked past. It is built into the walls themselves.
Completed: 2017
Construction cost:C$7.2 million (approx. $5.6 million USD), split between the Canadian government and private donors.
6. Reflections at Keppel Bay (Singapore)
Not every Libeskind project is a memorial. This luxury waterfront development—six curved glass towers between 24 and 41 storeys, demonstrates that the studio’s philosophy translates equally into the architecture of everyday life.
In a city defined by residential uniformity, the development was designed so that no two apartments across the entire complex share the same floor plan or view. Shifting angles, alternating orientations, and changing crown geometry give every home its own character. It is Libeskind’s argument, made in glass and steel, that people deserve to live in spaces shaped for them, not mass-produced around them.
Completed: 2011
Construction cost: Construction cost not publicly disclosed. The development sold 1,129 luxury apartments across a 750-metre waterfront site, with unit prices at the time of sale ranging from SGD $1.5 million to over SGD $10 million.
7. Złota 44 (Warsaw, Poland)
Warsaw was systematically destroyed by Nazi Germany during World War II, over 85% of the city razed. That it stands today, rebuilt and thriving, is one of history’s great acts of collective will. It was into this city that Libeskind returned to build his first major project in his birth country.
The 52-storey, 192-metre luxury residential tower’s sweeping glass facade curves upward in the shape of an eagle’s wing, Poland’s national emblem, representing freedom and sovereignty. Across the street, the heavy communist-era Palace of Culture looms. Złota 44 rises in direct contrast: light, fluid, and forward-looking.
Completed: 2016
Construction cost: Estimated €163 million (approx. $175 million) construction cost. The project faced severe financial difficulties; the original developer sold it midway through construction for just €50 million after significant losses.
8. Haeundae Udong Hyundai I’Park (Busan, South Korea)
Busan is South Korea’s second largest city and its largest port, a place whose identity is inseparable from the ocean. This waterfront development comprises three residential towers, the tallest reaching 72 storeys, alongside a hotel, offices, and retail.
Each tower was mathematically modelled to present a completely different silhouette depending on the angle of approach, the buildings seem to shift and breathe as you move around them. The curves draw on Korean natural tradition: ocean waves, wind-filled sails. The result is a large-scale modern complex that belongs unmistakably to the coastline it occupies.
Completed: 2011
Construction cost: Construction cost not publicly disclosed. The full 4.5-million-square-foot mixed-use development is one of the largest residential complexes in South Korea.
9. PwC Tower / CityLife Master Plan (Milan, Italy)
Part of a major regeneration of Milan’s historic fairgrounds, this 175-metre office tower, known locally as Il Curvo (The Curved One), tilts and arcs in a single clean geometric sweep from base to summit. In a skyline of vertical towers, its curve is immediately legible from across the city.
The design is a contemporary reinterpretation of the arcing forms found throughout Italian architectural history, translated into glass and steel. A building that speaks to where it stands rather than ignoring it.
Completed: 2020
Construction cost: Construction cost not publicly disclosed. The broader CityLife masterplan, encompassing three towers by Libeskind, Zaha Hadid, and Arata Isozaki, plus residential and retail, represents a total investment of over €2 billion.
10. Infinity Towers (Shanghai, China)
Currently under construction for the Lingang Group, these twin 100-metre commercial towers twist as they rise, their forms designed to evoke two dancing cranes, ancient Chinese symbols of longevity and wisdom, leaning toward each other mid-step.
The towers are connected at the 15th floor by a skybridge whose centre features a circular opening in the floor, looking directly down onto public water plazas below. It is a small gesture but a characteristic one: in a building designed to function, Libeskind finds the moment where structure, nature, and wonder briefly meet.
Completed: Under construction (expected completion not publicly confirmed)
Construction cost: Construction cost not publicly disclosed.
Other Notable Projects
Studio Libeskind has also designed the
Zhang Zhidong Museum (Wuhan, China)
Tikva Jewish Museum (Lisbon, Portugal)
Modern Art Center Vilnius (Lithuania)
Danish Jewish Museum (Denmark)
The Garden of Earthly Worries
The Wheel of Conscience Crystals at CityCenter (United States)
Bord Gáis Energy Theatre (Ireland)
Run Run Shaw Creative Media Centre (Hong Kong)
Ogden Centre at Durham University (United Kingdom)
Memoria e Luce 9/11 Memorial (Padua, Italy)
Albert Einstein Discovery Center (Ulm, Germany)
Together, these projects demonstrate Studio Libeskind’s defining conviction: that architecture is not a container for history, it is a way of making history felt. It is an approach that speaks directly to what Kigali will build at Gisozi.
Zhang Zhidong Museum.Albert Einstein Discovery Center in Ulm, Germany.
The concert will feature some of Rwanda’s leading artists, including Bruce Melodie, The Ben, Kitoko, and Bwiza.
Since the tour began, all performances have been streamed on Onstage.rw, where viewers can purchase access for 5,000 Rwandan francs and watch the full concert live from start to finish.
Amani Africa, who represents Artland, the company organising the tour in partnership with Watu Wave, said those unable to travel to Bugesera should not worry, as arrangements have been made to ensure they can still follow the event online.
He noted that lessons learned from the previous two concerts have helped improve the streaming experience, making it more reliable and enjoyable for viewers.
The Bugesera concert will be the third stop of the four-part Summer Country Tour, which began in Musanze on June 13, 2026, continued in Nyagatare on June 20, 2026, and will conclude on July 4, 2026, in Rubavu.
The concert has attracted a large number of music fans.Music fans attending the concerts continue to enjoy the experience.
The colorful event, held at Zaria Court on Friday evening, opened with an energetic performance by children from the Sherrie Silver Foundation, whose dance reflected the confidence and potential of a generation that has benefited from improved healthcare, education and protection.
The anniversary song was performed by UNICEF Champion Andy Bumuntu and brought to life through choreography by internationally acclaimed dancer Sherrie Silver, alongside children from her foundation. Their performance captured the voices and aspirations of young people determined to shape Rwanda’s future.
Over the past 40 years, UNICEF and the Government of Rwanda have worked together to improve child survival, expand immunization, strengthen maternal healthcare, increase school enrolment, improve nutrition and widen access to clean water and child protection services.
Through the anniversary campaign, UNICEF hopes to inspire renewed commitment from all sectors of society to continue investing in every child’s future.
Speaking during the celebration, UNICEF Rwanda Country Representative Lieke van de Wiel described the anniversary as a tribute to everyone who has contributed to improving children’s lives over the years.
“Today is about celebrating every partner, every family, every community and every young person who has helped shape a Rwanda where children have greater opportunities than ever before,” she said.
She added that she hopes the anniversary song will become part of children’s everyday lives.
“My dream is that children will be singing this song in schools while planting trees, in summer camps, on playgrounds and in their homes. When music becomes part of children’s daily lives, so too can the values of hope, unity and protecting every child’s future,” she said.
UNICEF Rwanda Country Representative Lieke van de Wiel addresses guests during the launch of the Rwanda@40 anniversary song, celebrating four decades of partnership in advancing children’s rights.
The celebration also unveiled several initiatives that will be implemented throughout the anniversary year, including the planting of 40 fruit trees in every primary school across Rwanda in partnership with government ministries.
UNICEF will also engage university students through nationwide competitions and dialogue sessions aimed at promoting children’s rights.
Minister of Youth and Arts Dr. Utumatwishima Jean Nepo Abdallah praised the long-standing partnership between Rwanda and UNICEF.
“For forty years, our partnership with UNICEF has helped ensure that more children begin life with hope and opportunity. Together we have chosen that every child receives healthcare, proper nutrition, quality education and protection,” he said.
While celebrating four decades of achievements, speakers emphasized that continued collaboration will be essential to address remaining challenges and ensure that every child in Rwanda has the opportunity not only to survive, but also to thrive and fulfil their potential.
Minister of Youth and Arts Dr. Utumatwishima Jean Nepo Abdallah speaks during the UNICEF Rwanda@40 celebration, reaffirming the country’s commitment to improving the lives of every child.Children from the Sherrie Silver Foundation perform during the launch of UNICEF Rwanda’s 40th anniversary song,Outstanding schools receive awards during the UNICEF Rwanda@40 anniversary celebration, acknowledging their efforts in supporting children’s learning and wellbeing.
The decision was announced on Friday evening, June 26, 2026, in a statement read on national television by the military government of Captain Ibrahim Traoré, who has led the country since September 2022.
“The government of Burkina Faso hereby informs the national and international community that it has decided to sever diplomatic relations with France with effect from today, June 26, 2026,” Communications Minister Pingdwende Gilbert Ouédraogo stated.
Ouédraogo said the move followed a thorough review of bilateral relations, concluding that the “essential conditions for promoting relations based on mutual respect, reciprocal trust, respect for the principle of non-interference in internal affairs and national sovereignty are not in place.”
The junta went on to accuse Paris of persistent activism against Burkinabè interests, accusing it of “blatant neo-colonial ambitions” and active support for “subversive networks and terrorists” operating within the region.
Paris responds
France responded swiftly to the announcement through its Ministry of Foreign Affairs, firmly rejecting the accusations and condemning the move.
French Foreign Ministry spokesperson Pascal Confavreux denounced the immediate cutoff as a “hostile and unfounded decision.” In an official statement, Paris noted that the development “illustrates the worrying drift of the Burkinabè authorities.”
Confavreux added that France is actively monitoring the safety of its diplomatic personnel and French citizens remaining in the country, urging expatriates to exercise heightened vigilance. Furthermore, the ministry signaled a firm diplomatic counter-response, stating that “necessary reciprocal measures are currently under review.”
People-to-people ties preserved
In its initial statement, the Burkinabè government emphasised that the complete break concerns only the formal institutional framework between the two states.
“This decision exclusively concerns diplomatic relations between the two states and does not call into question the historical, human, cultural and social ties between the people of Burkina Faso and France,” the communiqué read.
Ouagadougou added that French nationals residing in Burkina Faso would continue to be protected in accordance with national laws, calling on citizens to show responsibility, restraint, and civic-mindedness toward expatriates.
Burkina Faso has been battered by a grueling security crisis for more than a decade, with armed extremist groups linked to Al-Qaeda and the Islamic State operating across its territory and the wider Sahel region. The ongoing conflict has caused thousands of deaths and displaced millions of people.
Relations between Paris and several Sahelian capitals have imploded in recent years. Following successive military coups, regional governments have aggressively reassessed their traditional political, military, and diplomatic reliance on the West.
France, which long maintained extensive post-colonial influence in West and Central Africa, already withdrew its military forces and suspended development aid to Burkina Faso in 2023.
This formal diplomatic break aligns with a broader foreign policy shift by the Alliance of Sahel States (AES), comprising Burkina Faso, Mali, and Niger, as they pivot away from traditional European partnerships to diversify international cooperation and strengthen ties with emerging global powers.
Burkina Faso has announced the immediate severance of diplomatic relations with France, marking a definitive rupture in the relationship between the West African country and its former colonial ruler.
Addressing a Congolese audience alongside President Félix Tshisekedi, Ndayishimiye declared: “You must have confidence that you have a common enemy. When you have a common enemy, to fight it, unity is required.”
There is little doubt that this message is directed against Tutsi communities, particularly the Banyamulenge and other Congolese Tutsi populations who have long faced discrimination, exclusion, and violence in eastern DRC.
The context only reinforces this interpretation: Burundian forces are currently operating alongside a coalition that includes the Armed Forces of the DRC (FARDC), the FDLR genocidal group, Wazalendo militias, and foreign mercenaries.
Ndayishimiye’s remarks are neither a message of reconciliation nor de-escalation. On the contrary, they directly undermine diplomatic efforts led by the United States, Qatar, and the African Union.
The Washington peace agreement between Kigali and Kinshasa, as well as ongoing discussions between the Congolese government and the AFC/M23, are centered on peaceful conflict resolution and political dialogue, not military confrontation. Yet Ndayishimiye’s intent is to stir conflict and incite further violence against Congolese Tutsi communities.
Ndayishimiye’s remarks are neither a message of reconciliation nor de-escalation.
Shortly after his meeting with Tshisekedi, Ndayishimiye recommitted to sending several hundred additional Burundian troops to the DRC. This development coincides with reports that the FARDC-FDLR-Burundian coalition is reorganizing following recent battlefield setbacks. Military units are reportedly being reassembled around Minembwe, Kamanyola, and the Rusizi Plain, potentially in preparation for renewed large-scale operations.
Ndayishimiye has increasingly positioned himself as a central actor in policies and military actions that contribute to the marginalization and displacement of Tutsi communities in eastern DRC. Burundi has already deployed more than 20,000 troops, operating primarily in South Kivu, including Fizi, Mwenga, and areas surrounding Minembwe.
Concerns regarding Ndayishimiye’s stance toward the Congolese Tutsi, or Banyamulenge, are not new. In previous statements, he questioned the existence of the Banyamulenge as a distinct ethnic community, arguing that they lack a traditional chieftaincy, a claim that is historically inaccurate and politically significant, as it challenges the identity and legitimacy of a community that has lived in the region for centuries.
The Burundian president has also argued that the Banyamulenge issue emerged only after Rwanda’s intervention in Zaire in 1996. Historians and regional experts dispute this characterization, noting that disputes over the citizenship, identity, and political status of the Banyamulenge long predate the wars of the mid-1990s. The roots of these tensions stretch back decades and are deeply intertwined with colonial-era policies, questions of nationality, and local power struggles.
Ndayishimiye’s reference to a “common enemy” carries significant weight. In a region where ethnic tensions have repeatedly fuelled cycles of violence, such language cannot be interpreted as a simple call for unity. Instead, it reinforces narratives that portray entire communities as threats, inciting ethnic violence at a moment when political dialogue and reconciliation are urgently needed.
As peace initiatives continue to gain international support, the key question remains: will regional leaders pressure the Ndayishimiye-Tshisekedi alliance to embrace inclusive political solutions, or will they stand by as military escalations continue and eventually spiral out of control?
Shortly after his meeting with Tshisekedi, Ndayishimiye recommitted to sending several hundred additional Burundian troops to the DRC. This development coincides with reports that the FARDC-FDLR-Burundian coalition is reorganizing following recent battlefield setbacks.
The discussions focused on the ongoing work towards the East African Political Confederation, with particular attention to progress on drafting its Constitution and the next steps in advancing the regional integration agenda.
The meeting comes as the EAC continues region-wide consultations on the proposed Political Confederation, a transitional arrangement adopted by Heads of State in 2017 as a pathway towards the eventual Political Federation of East African States.
In Rwanda, the consultations were launched on June 15 and were conducted across different parts of the country, including Kigali, Rubavu, Huye and Nyagatare. The two-week exercise, which concludes on June 27, is aimed at gathering citizens’ and stakeholders’ views to inform the drafting of the Constitution of the Political Confederation.
The consultations have brought together participants from government institutions, Parliament, the judiciary, academia, civil society, the private sector, youth and women’s groups, faith-based organisations, persons with disabilities, political parties and the media.
According to the EAC Secretariat, the views collected across Partner States will inform the development of the governance framework of the Political Confederation and help define institutional structures for the next phase of regional integration.
EAC officials describe the process as a key milestone in the broader integration agenda, which also includes the Customs Union, Common Market, and ongoing implementation of the Monetary Union Protocol, as Partner States work towards deeper economic and political integration.
Speaking during earlier phases of the consultations, EAC officials emphasized the importance of citizen participation in shaping the integration framework.
“This is not merely an exercise. The Treaty is very clear that the Community is people-centred, and therefore, citizens must be consulted when major decisions about our integration are being made,” said EAC Secretary General Ambassador Stephen Mbundi.
President Paul Kagame hosted the EAC delegation at Urugwiro Village.The discussions focused on the ongoing work towards the East African Political Confederation, with particular attention to progress on drafting its Constitution and the next steps in advancing the regional integration agenda.
Hall, who has built a global following through viral, high-intensity fitness routines, recently teased the trip on his social media platforms.
In a series of clips showing him racing against cars and aircraft, the influencer repeatedly exclaimed “Africa,” signaling his forthcoming visit to the continent. He also shared a sequence of national flags outlining his planned itinerary, confirming that the tour will begin on June 28, 2026.
As part of the tour, Hall is expected to visit a series of African countries, including Algeria, Angola, Benin, Botswana, the Democratic Republic of the Congo, Burundi, Uganda, and South Africa, among others.
The 30-year-old influencer is known for his disciplined daily fitness regimen, typically carried out in the early morning hours. He says he has maintained this routine consistently for the past 15 years.
His upcoming African tour follows previous international visits to countries such as Germany, Puerto Rico, India, and the United Arab Emirates, where he has often collaborated with local creators and fitness enthusiasts.
In Rwanda, social media personality Kagarara has been among those inspired by Hall’s style of content creation. He began producing similar content after meeting American streamer IShowSpeed, who previously visited Rwanda.
Hall, who has built a global following through viral, high-intensity fitness routines, teased the trip on his social media platforms.The 30-year-old influencer is known for his disciplined daily fitness regimen, typically carried out in the early morning hours. He says he has maintained this routine consistently for the past 15 years.
Led by Chief Executive Officer Romeo Ngarambe, the delegation held talks with the Nigerian Exchange Group and the Central Securities Clearing System in Lagos, drawing lessons from one of Africa’s largest capital markets.
At the Nigerian Exchange Group, the delegation met Jude Chiemeka, Chief Executive Officer of Nigerian Exchange Limited, and Temi Popoola, Group Managing Director and Chief Executive Officer of NGX Group. The discussions covered market regulation, trading systems, investor access and opportunities for closer links between African exchanges.
The institutions also examined cooperation through the African Securities Exchanges Association and the African Exchange Linkage Project, which is designed to enable investors to access securities listed across participating markets.
Greater cross-border market access could widen the pool of investors available to Rwandan companies, support capital raising and improve the movement of investment funds between African economies.
During discussions with the Central Securities Clearing System, the delegation reviewed Nigeria’s experience in securities depository services, settlement-cycle reform, market dematerialisation, risk management and post-trade technology.
The engagement included lessons from Nigeria’s move to a T+1 settlement cycle, where securities transactions are completed one business day after trading. Faster settlement can reduce transaction risks, improve market efficiency and allow investors to access their securities and funds sooner.
Ngarambe said cooperation between African institutions was essential to building stronger and more accessible markets.
“African capital markets can grow faster when institutions share experience and adapt solutions that have worked on the continent. Our objective is to build efficient, trusted and accessible market infrastructure that supports investment in Rwanda and regional integration,” he said.
The delegation also held engagements with Nigeria’s Securities and Exchange Commission and Debt Management Office.
CMA Rwanda said lessons from the mission would support ongoing efforts to strengthen supervision, improve market infrastructure, expand investment products and attract domestic and international investors.
The cooperation is expected to contribute to a more connected African capital market in which businesses can access long-term financing and investors can participate in opportunities beyond their domestic markets.
The mission, led by CMA Chief Executive Officer Romeo Ngarambe, took place in Lagos where the delegation held engagements with key Nigerian financial market institutions
The exhibition, which opened on Thursday, has also brought together more than 30 Rwandan coffee companies involved in coffee processing, exporting, and trading.
World of Coffee serves as a global platform where coffee producers, traders, buyers, and industry professionals exchange knowledge, explore new business opportunities, and strengthen partnerships.
For Rwanda, the event offers an important opportunity to expand export markets while showcasing the exceptional quality of Rwandan coffee to an international audience.
The three-day exhibition is being held at Brussels Expo and will conclude on June 27, 2026.
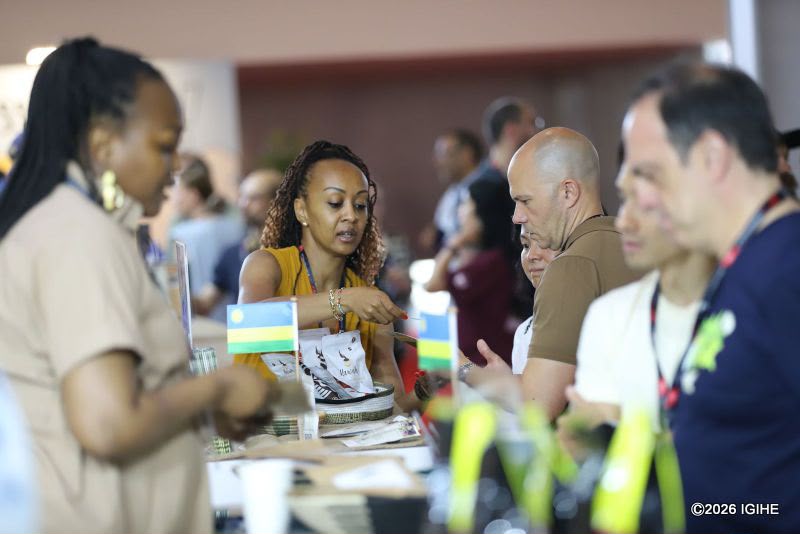
Thousands of participants from across the world, including coffee farmers, exporters, roasters, buyers, investors, and industry experts, are attending the event.
This marks the first time that World of Coffee has been hosted in Belgium.
Throughout the exhibition, participants will take part in business meetings, panel discussions, coffee tastings, international competitions, and networking sessions designed to foster collaboration across the global coffee sector.
Rwanda’s participation is part of its broader strategy to strengthen its position among the world’s leading producers of high-quality specialty coffee.
The country is showcasing the expertise of its coffee farmers, processors, cooperatives, and exporting companies, all of which play a vital role in the growth of Rwanda’s coffee industry and the national economy.
Europe remains Rwanda’s largest coffee export market, accounting for about 60% of total shipments, making the Brussels platform particularly important for deepening existing trade links and exploring new premium opportunities.
The participation comes at a time when Rwanda’s coffee sector is experiencing strong growth, generating a record $148.6 million in export revenues in 2025, a 65% increase compared to the previous year.
Photos from the opening day of the exhibition:
More than 30 Rwandan coffee companies involved in processing, exporting, and trading are participating.
World of Coffee serves as a global platform where coffee producers, traders, buyers, and industry professionals exchange knowledge, explore new business opportunities, and strengthen partnerships.For Rwanda, the event offers an important opportunity to expand export markets while showcasing the exceptional quality of Rwandan coffee to an international audience.